
Learning to Solve Big Problems

The Problem
Emergency patients that arrive to the Mater Emergency Department (ED) are rapidly triaged, assessed and urgent treatment commences as appropriate. However, non-emergency patients routinely end up in ED as well, even though this is not the optimal place for their care. These avoidable and unnecessary attendances slow the flow in ED and increase demand on an already stretched ED. They consume resources unnecessarily such as acute beds, emergency trained staff, ancillary staff, diagnostics and other services.
The Mater Hospital Transformation Office, Emergency Department staff and hospital management facilitated my MA Interaction Design class and our MA Service Design student colleagues to conduct a 5 week long 'live project' to intensely research, analyse and develop viable solutions to address the issues with avoidable attendances to ED. Successful outcomes would have the potential to aid in addressing the going national Emergency Department overcrowding crisis.

The Challenge
We need to better understand why this happens:
● What is it about the systems and structures that incentivises this?
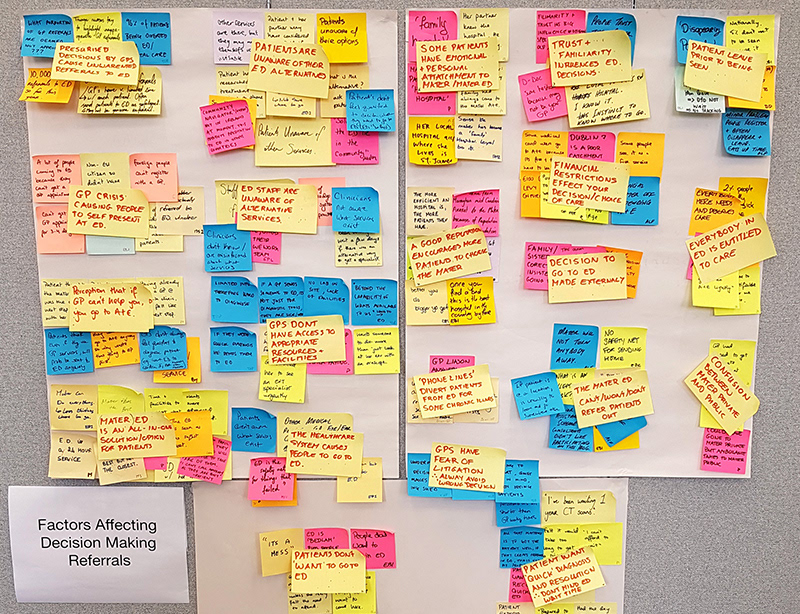
● What influences the decision to present to or refer to ED – for patients, carers and healthcare professionals?
● What’s the best mechanism to streamline patients to the most appropriate service?
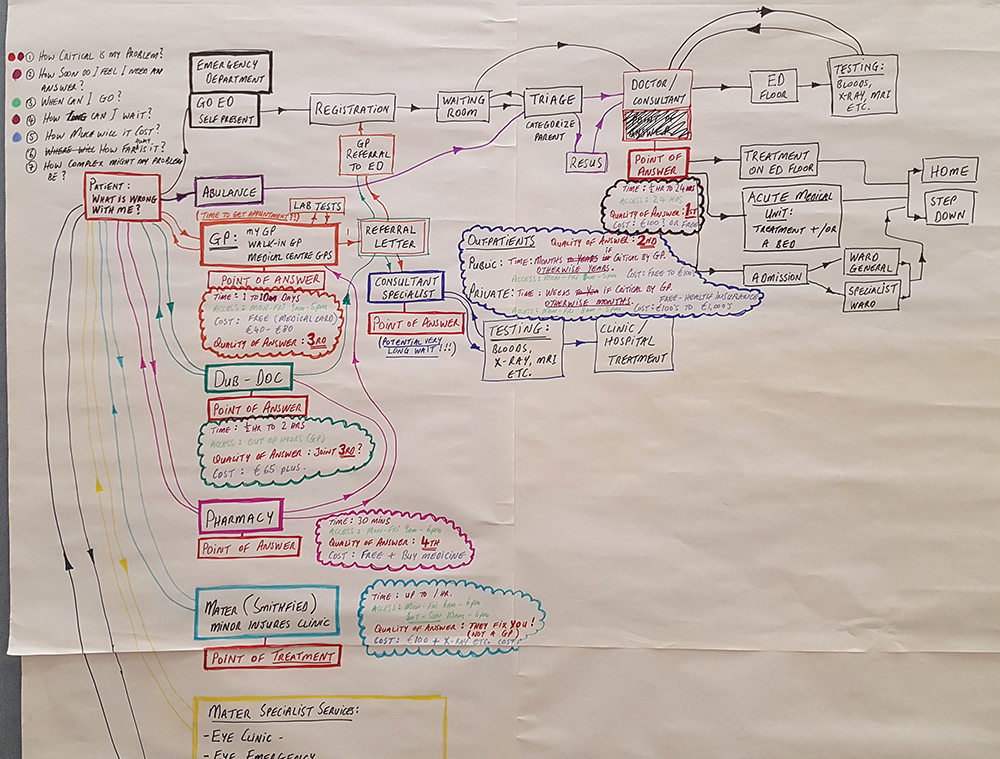
● What are the key decision points and how might we influence decision makers at these critical junctures?
● What is it about the systems and structures that incentivises this?
● What influences the decision to present to or refer to ED – for patients, carers and healthcare professionals?
● What’s the best mechanism to streamline patients to the most appropriate service?
● What are the key decision points and how might we influence decision makers at these critical junctures?

Project Approach
We would respond to the brief as a collective design team, working independently, in small groups and as part of an overall team at different stages of the project. Our response to the brief was required to be grounded in strong human-centred research and insights.
We would immerse ourselves in research in order to fully interrogate the brief. Following this deep dive research phase we would work to extract meaning and insights from the data gathered, presenting a collective view of the research. Moving from research to concepts we would form into smaller project groups.
The project placed an emphasis on user engagement throughout the process from research, through concept generation, prototyping and delivery of final design outcomes. We would then execute and resolve your project through iterative prototyping and testing in the real-world with the key stakeholders and users.
Research Phase





In teams we conducted, analysed and synthesised both primary and secondary research and working as a studio we came together to make sense of our research. We conducted patient interviews, expert interviews, guerrilla interviews in various locations and carried out observation studies in the ED. Through workshops we unpacked all this initial research and planned necessary additional research. We interviewed all key staff and management stakeholders and conducted fieldwork in the Emergency Department via research relays to interview patients and staff alike with the aid of questionnaires, study the environment and examine the processes taking place.
Research Presentation at the Mater


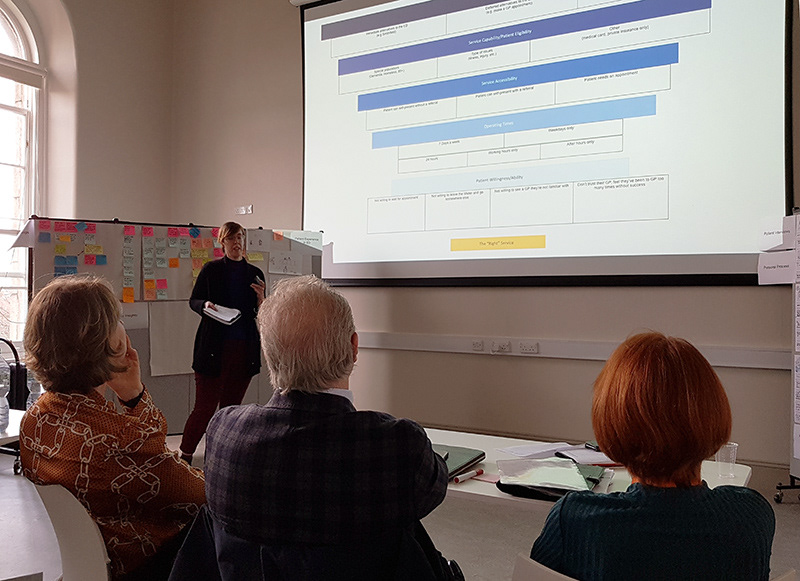
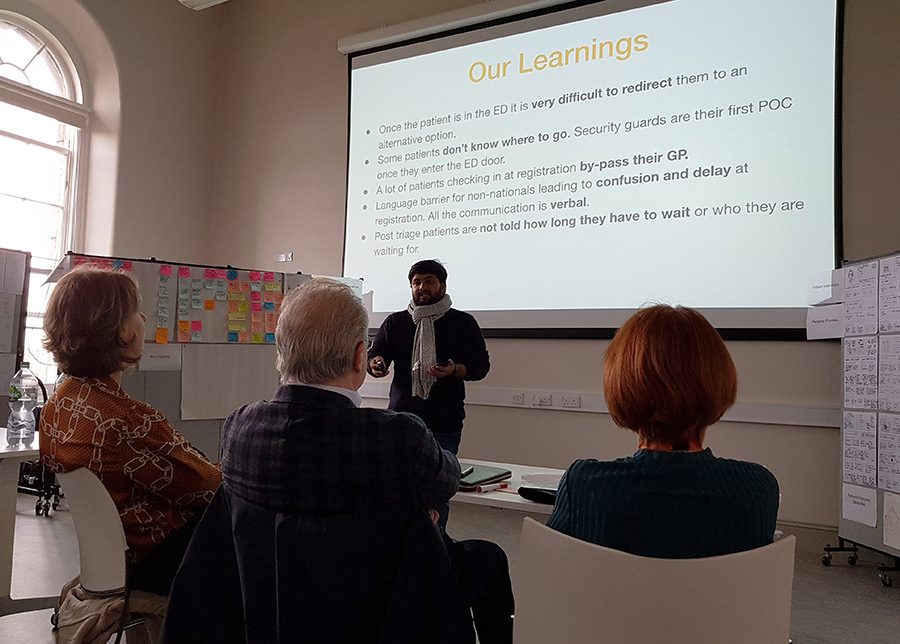



Collectively we presented our research finding in detail to a panel of hospital and ED management covering the following areas:
• Research process
• Areas of investigation
• Key findings
• Design insights
• A range of opportunities for intervention
• Research process
• Areas of investigation
• Key findings
• Design insights
• A range of opportunities for intervention
A variety of data analysis methods were used to present our findings in visual form to the panel. Data was transformed to Post-It note pieces of data. Iterative 'clustering' and 'affinity maps' helped us make key findings and design insights. Sketch 'personas' were developed to show groups of users and 'user-flows' helped to high-light patient decision making.
Initial Concept Idea Exploration




After the Research Phase, we broke into small teams of 3 and each team now focused on an specific area in investigation to initiate a range of concepts in response to the particular area of the research findings. These little teams now worked together for the remainder of the project.
Our team: Sarah Heffernan, Ryan Williams and myself.
Our area of investigation and concept generation: how to impact patient decision making in advance to them presenting at ED so that they can find to most appropriate healthcare service for their medical need.
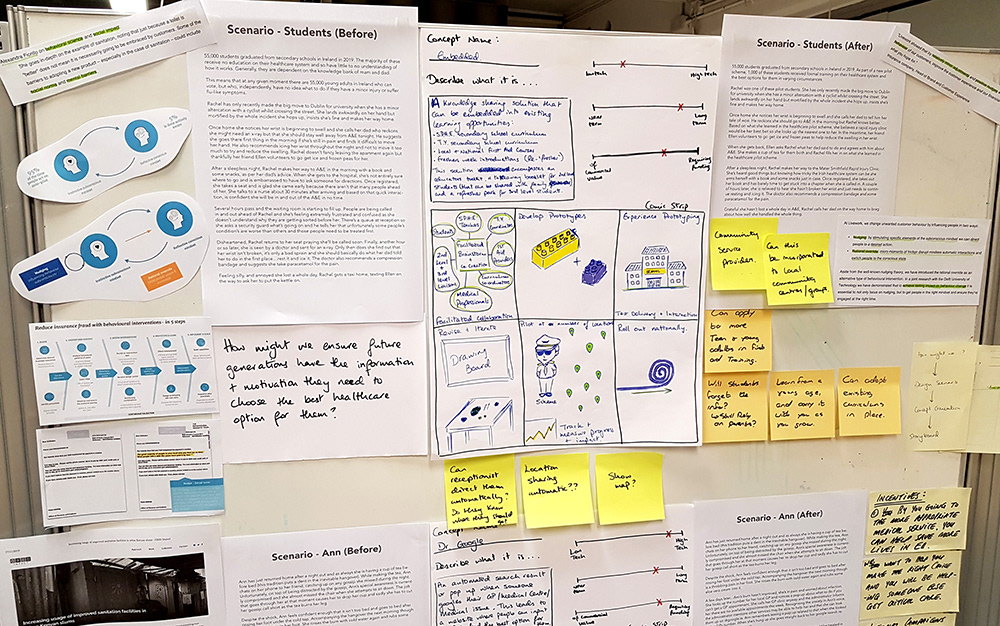
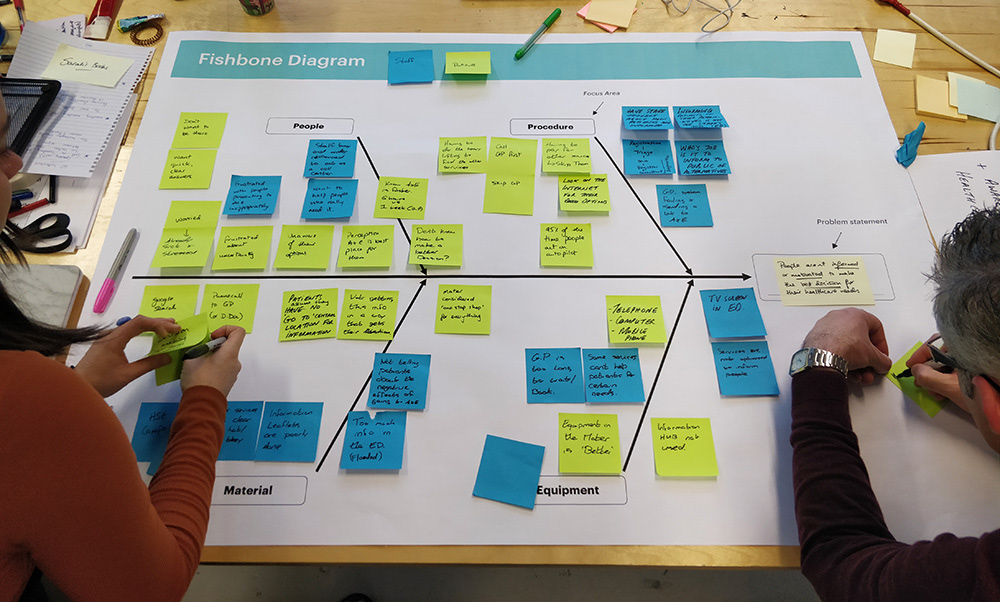
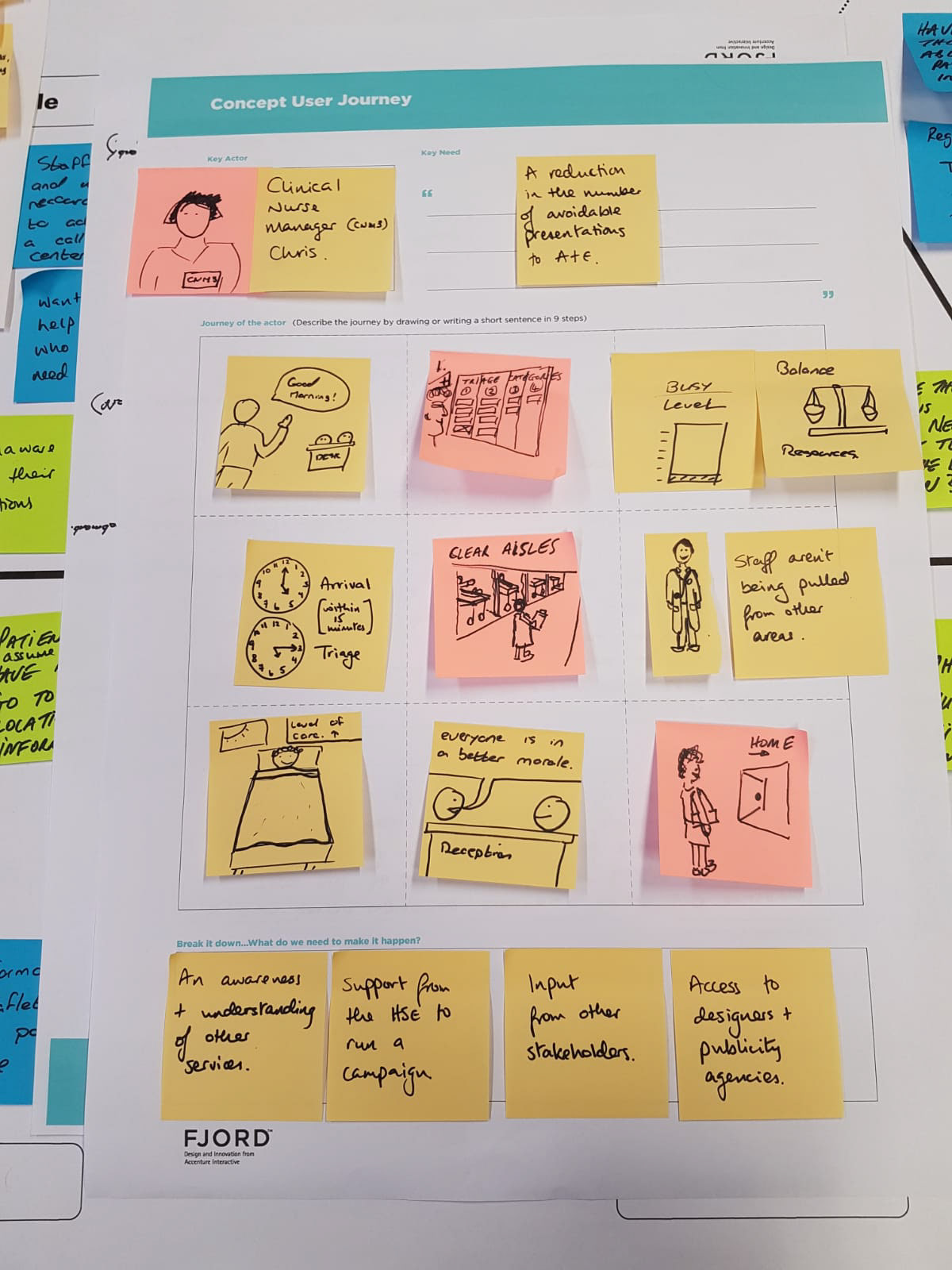
Concept ideas were generated by brainstorming, storyboarding, using fishbone diagrams, user journey maps and building 'before' and 'after' scenarios to explore the potential opportunities. An initial draft concept presentation was given in studio to fellow students, tutors and hospital panel member to help shortlist our concepts.
Concept Visualization


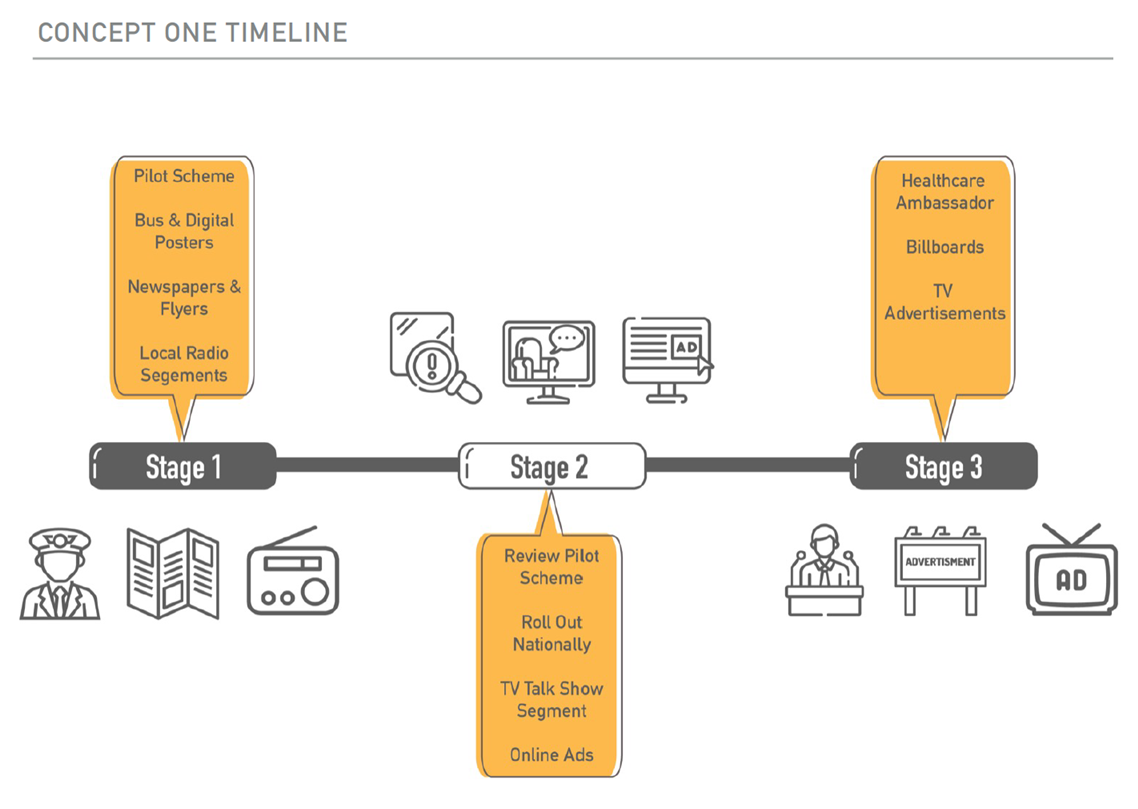
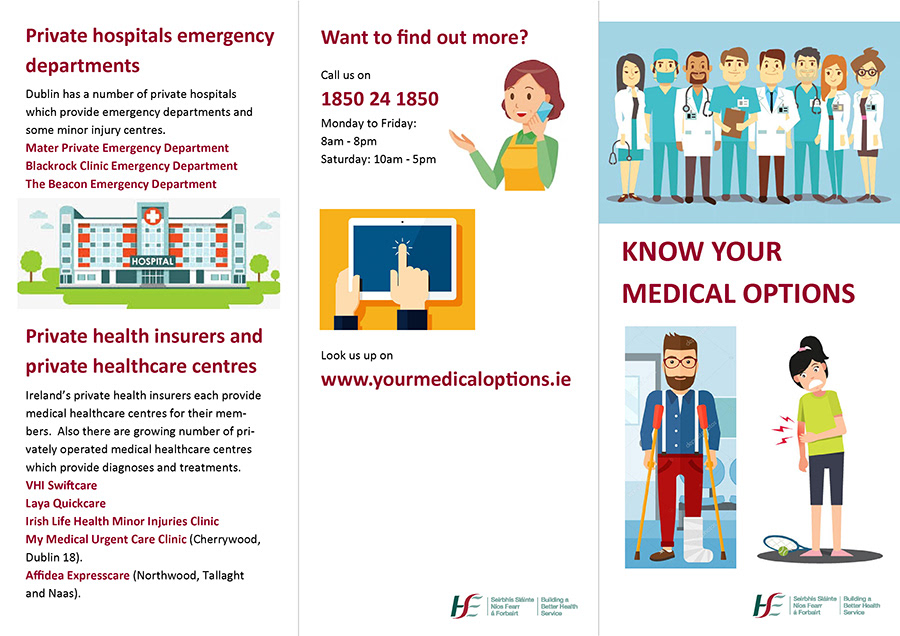
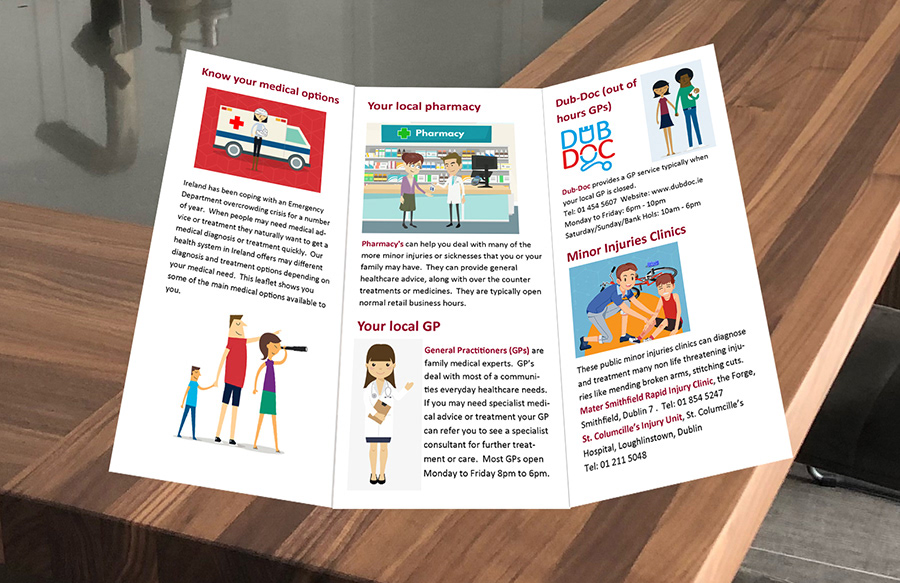

Following the draft concept presentation, we then focused on two key concept areas; a local and national awareness campaign promoting the availability of alternative services, and an educational piece to inform 2nd and 3rd students about how to make the best healthcare choices for their future medical needs (early interventions). We produced some visual concepts and prototypes to demonstrate our ideas.
Concept Presentation at the Mater



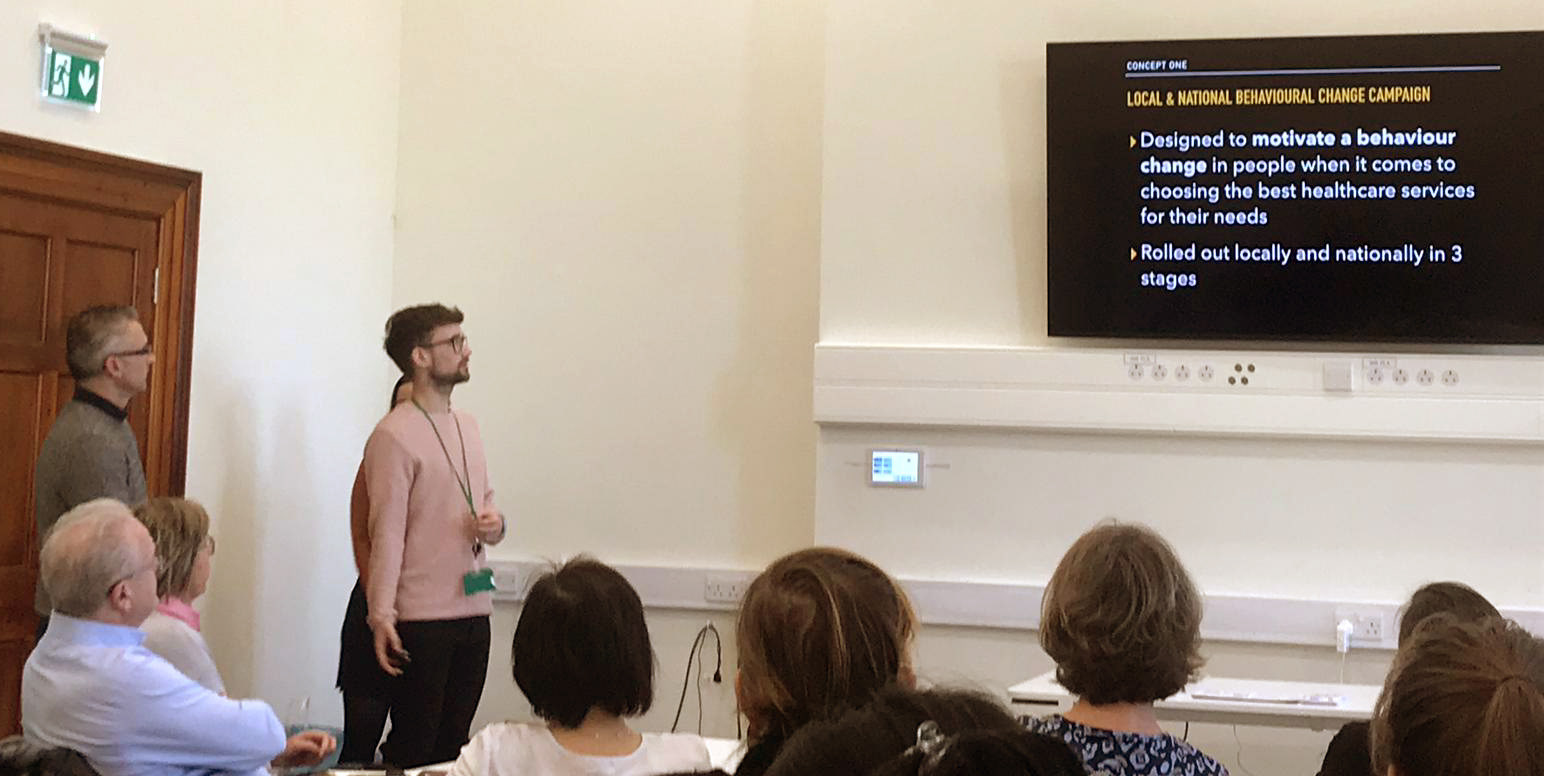
We then presented out completed Concept Presentation to our panel of hospital and ED management for critical feedback. Following this presentation we had the opportunity to meet with national health awareness campaign department for the HSE. We were able to discuss the real-life role out of previous national health campaigns regarding our concept to promote alternative healthcare services. We gained some very valuation insights that part of their essential criteria for rolling out campaigns are that appropriate fully functioning service infrastructure must first be in place before promoting it. As this was currently not the case, a campaign to promote alternative healthcare services would not recommended at this point. With these newly gained expert insights our team decided to move forward with the 2nd and 3rd level educational concept direction.
Prototyping and Testing Final Designs
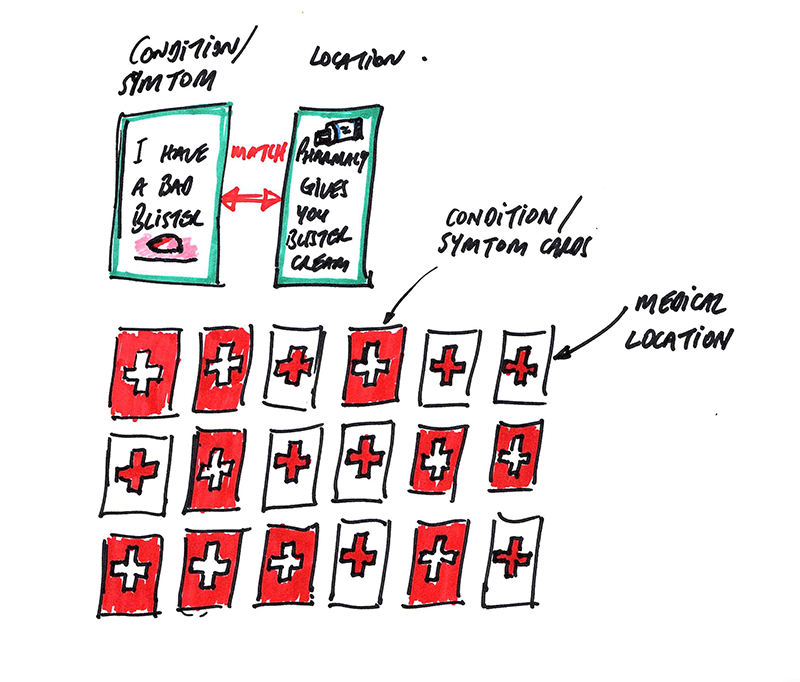
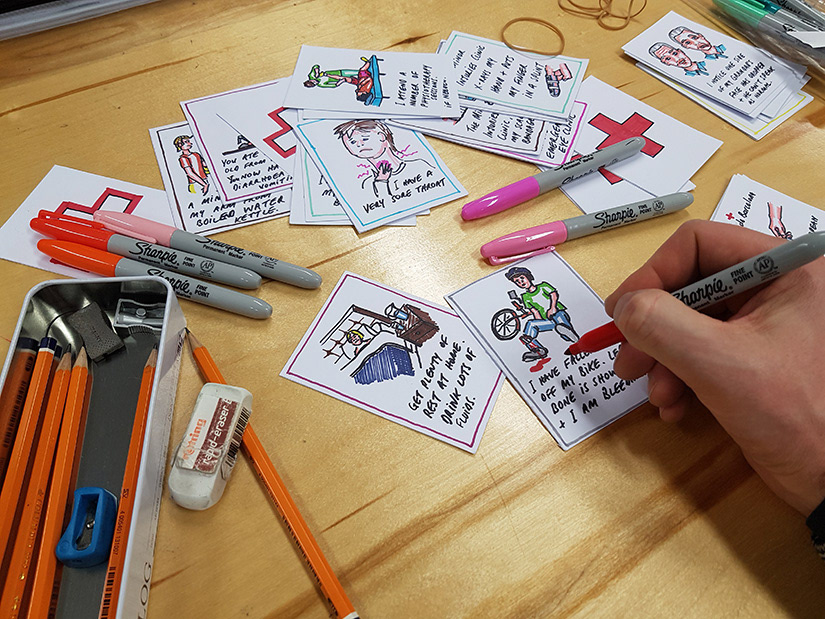
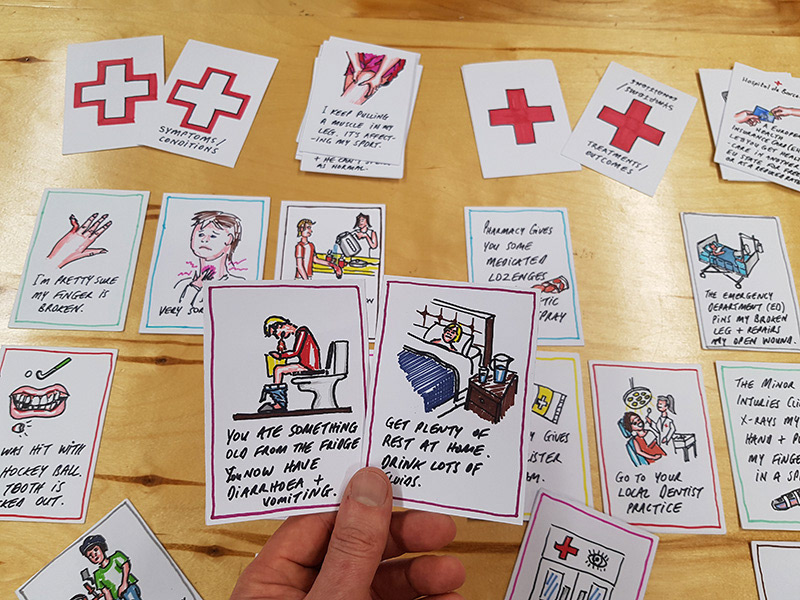
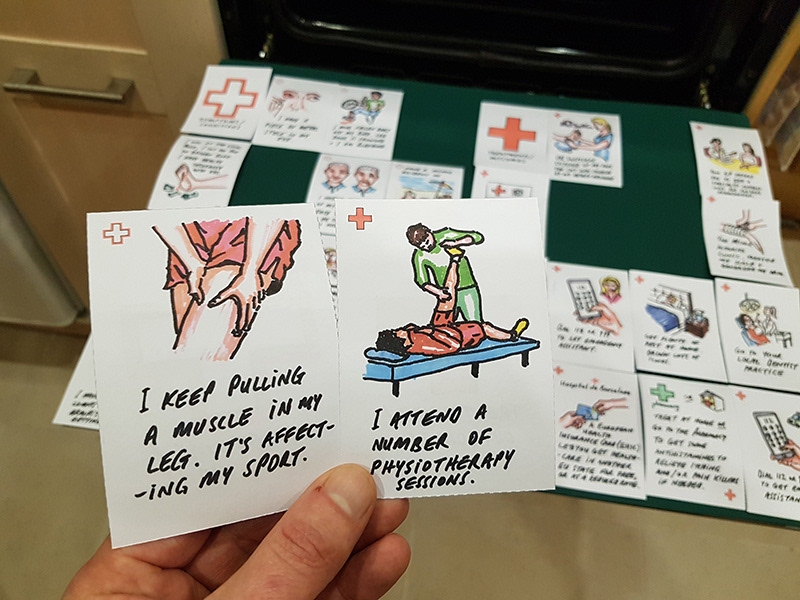
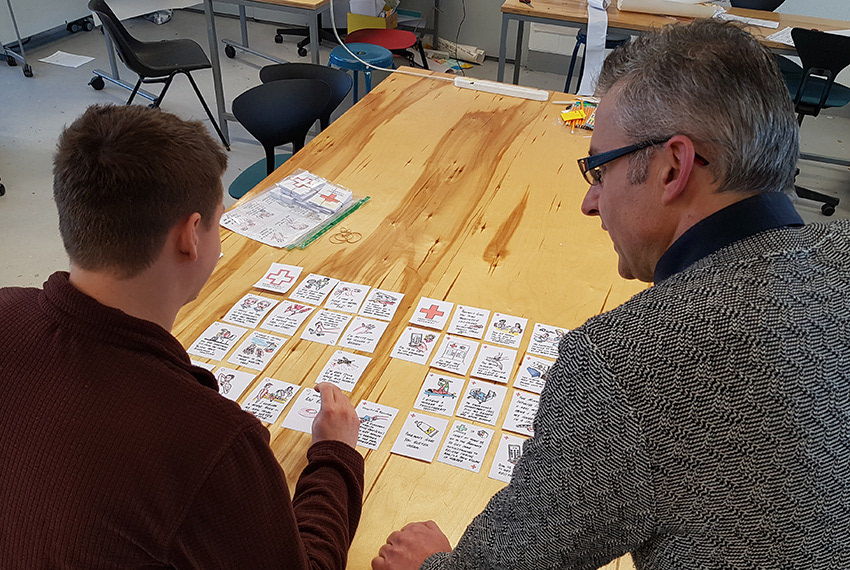
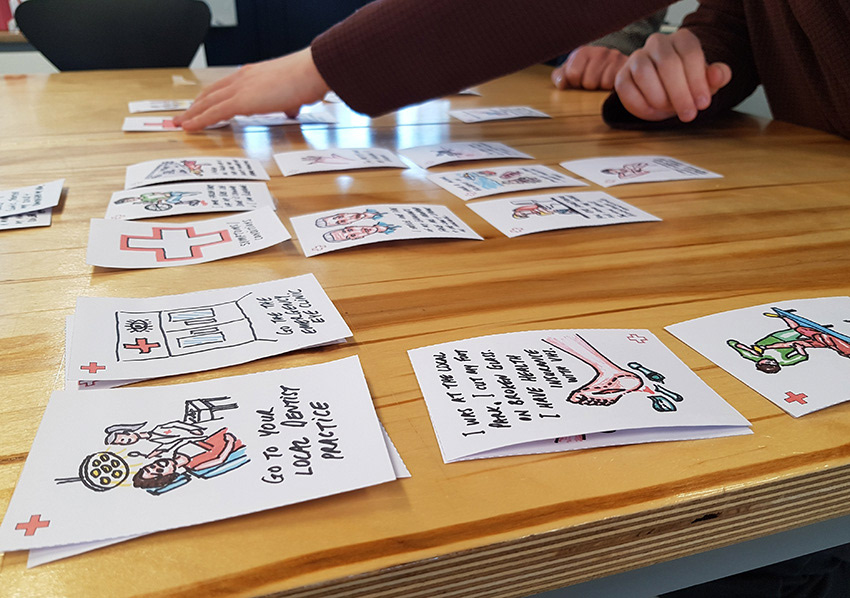
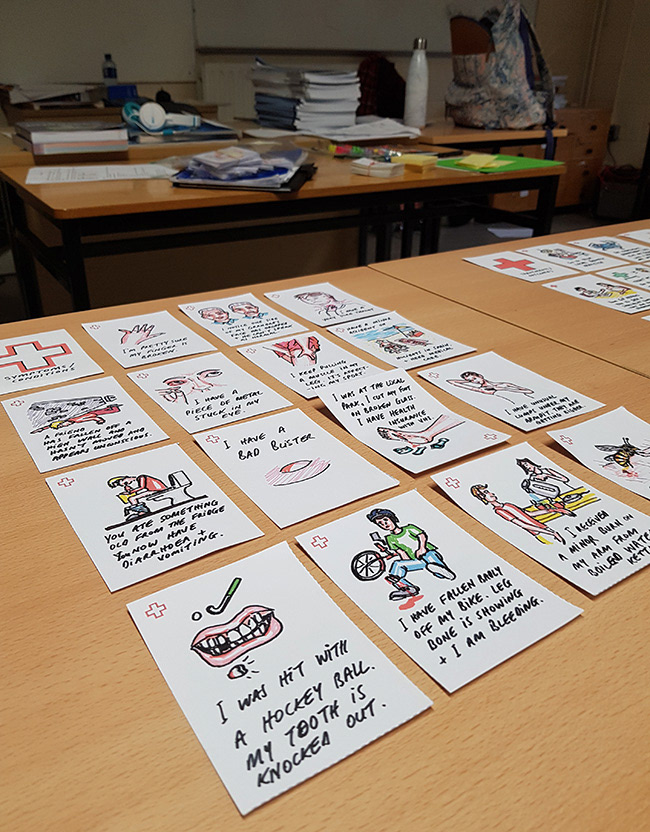

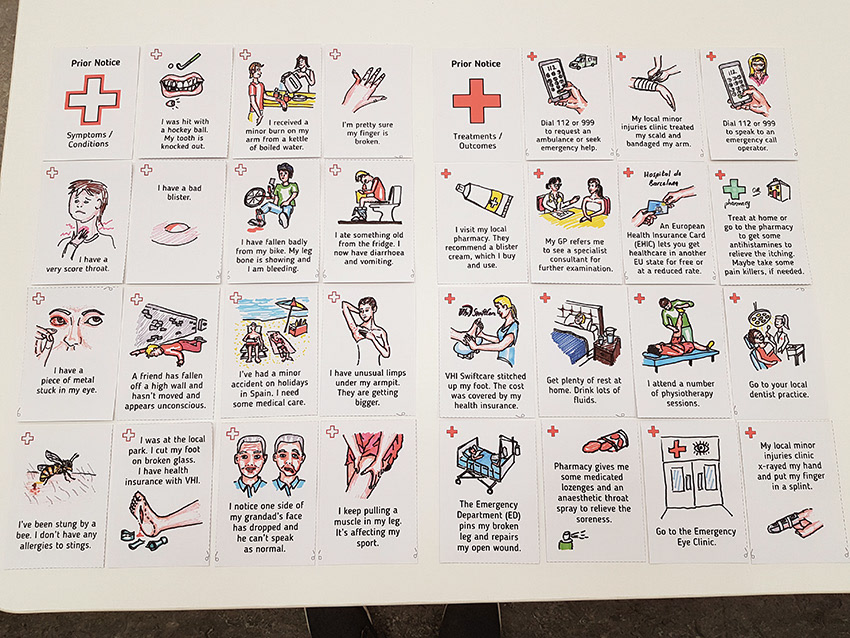
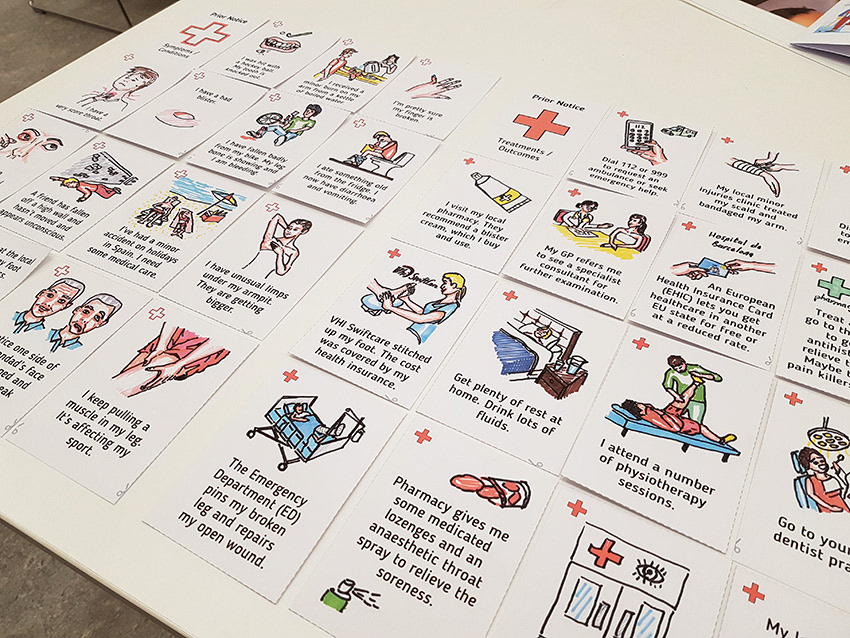
After numerous rounds of iterative prototyping and testing I developed an educational playing card game that students would play buy matching the 'symptoms or conditions' with the appropriate 'treatments or outcomes'. The game has packaged into an easy to use format for educators / teachers. You downloaded the PDF, printed the pages on 2 sides and simply cut out the cards to create the game. The game encouraged conversation while educating the students about the most appropriate healthcare service to use for different medical scenarios. This and other items that formed part of an educational toolkit would help give students prior knowledge of our health services.